
Massive haemmorhage is one of the leading causes of death in motor vehicle related trauma, and with only minutes to death from a significant arterial bleed, the reality is that a percentage of salvageable casualties will die from potentially compressible bleeds prior to emergency services arriving. The authorities in the United States have recognised this fact in regard to active shooter scenarios and terrorist mass-casualty incidents, and have instituted the bystander Stop The Bleed campaign aimed at empowering the civilian first-responder to such a scenario to save lives (HomelandSecurity 2015).

Whilst an active shooter event or mass-casualty terrorist incident remains an unfortunate possibility in our current world climate, a far more likely instance in which the life-saving skills of massive haemmorhage control might be required is a motor vehicle accident.
As per the Stop The Bleed infographic above, if external bleeding can be seen, and you have decided to act to stop it (considering the danger of the situation and risk of potential blood-borne virus exposure) the initial technique is firm direct pressure to the wound. Research shows that the maximal pressure achievable with a firm pressure dressing will be around 90mmHg (Naimer 2000), which will be enough to control most bleeding from the low pressure venous system, however if the bleeding is from a severed artery, a pressure dressing alone may not be enough to stop it. Normal peak pressures in the arteries of an adult range from 120-140 mmHg, and under duress or in pain, such as a casualty situation, may exceed 200 mmHg. Looking at those numbers it can be seen that a firm pressure dressing may be inadequate to control bleeding, and an arterial tourniquet might be appropriate. This tourniquet should be placed around 5-10cm (2-4 inches) above the level of the injury on an arterially bleeding limb.
If a commercially made arterial tourniquet is available then the problem is solved fairly easily by the skilled first-responder by following the steps below:

The life-saving application of an arterial tourniquet by two appropriately trained Police Officers can be seen in the video below.
Photo source: https://www.reddit.com/r/news/comments/1cen3t/there_was_just_an_explosion_at_the_boston
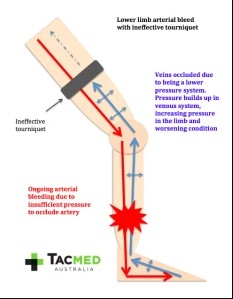
No discredit is intended to the first responders at the Boston Marathon, and their rapid and decisive actions in treating and evacuating the wounded unquestionably saved many lives. The issue however with applying an improvised tourniquet to a limb which cuts off the venous system but is not tight enough to occlude the arterial system is that blood will continue to flow into the injured limb, and hence the wound will continue to bleed, and the remaining blood will be trapped in the limb as illustrated below. This has the unwanted effect of increasing the pressure in the injured limb and actually worsening the prognosis for the casualty.
Research has demonstrated that 99% of improvised tourniquets without a windlass will fail to effectively stop arterial bleeding (Altamirano MP 2015), and even with a windlass around 30% of tourniquets will fail (Altamirano MP 2015). The choice of improvised windlass is also crucial, as items such as pencils and small craft sticks have been demonstrated to break 75-80% of the time before sufficient pressure has been applied to a tourniquet to occlude arterial blood flow (Kragh JF 2015).
With all of that in mind I wanted to see whether I could improvise an effective tourniquet from items that I had in the boot of my car, to simulate common things that would be readily at hand in a car crash scenario.
Using a length of an old towel and a jack handle I was able to fabricate an improvised arterial tourniquet and within 45 seconds occlude the blood flow to one of my legs with it (proven by an absence of palpable foot pulses). The technique was as follows:



I certainly appreciate that as a trial of one, done on myself, this experiment holds no scientific credibility (for the science behind improvised tourniquets please see Altamirano et al. 2015 and Kragh et al. 2015). This was not the point of the exercise, it was simply to demonstrate that an effective arterial tourniquet could be rapidly fabricated and applied in a car crash scenario with items that would be readily available. The goal of this article is to seed the thought in the reader’s mind of what might be used to fabricate an effective tourniquet in an extreme situation where commercially available medical equipment is not at hand. The choice of equipment used for an improvised tourniquet is almost limitless, however for it to have the best chance of working, a tight band of ideally 5cm (2 inches) width needs to be created around the limb, approximately 5-10cm (2-4 inches) above the site of arterial bleeding, and a windlass of appropriate strength must then be used to tighten the device. The windlass must then be held under tension until emergency services arrive to take over, or an effective solution to locking it in place can be fabricated. It must be noted that this improvised tourniquet was extremely painful when applied to the tension required to occlude arterial flow. The use of such an improvised device would be in extremis only, however when the chips are down, having the skills to fabricate and apply one might just save a life!
Of course a better solution to the problem would be to have an appropriately stocked car medical kit. For the contents of such a kit, as compiled by a former Special Operations and current TacMed Australia colleague of mine, please click on this link.
As always, comments and questions are welcome.
Kind regards, dan pronk